
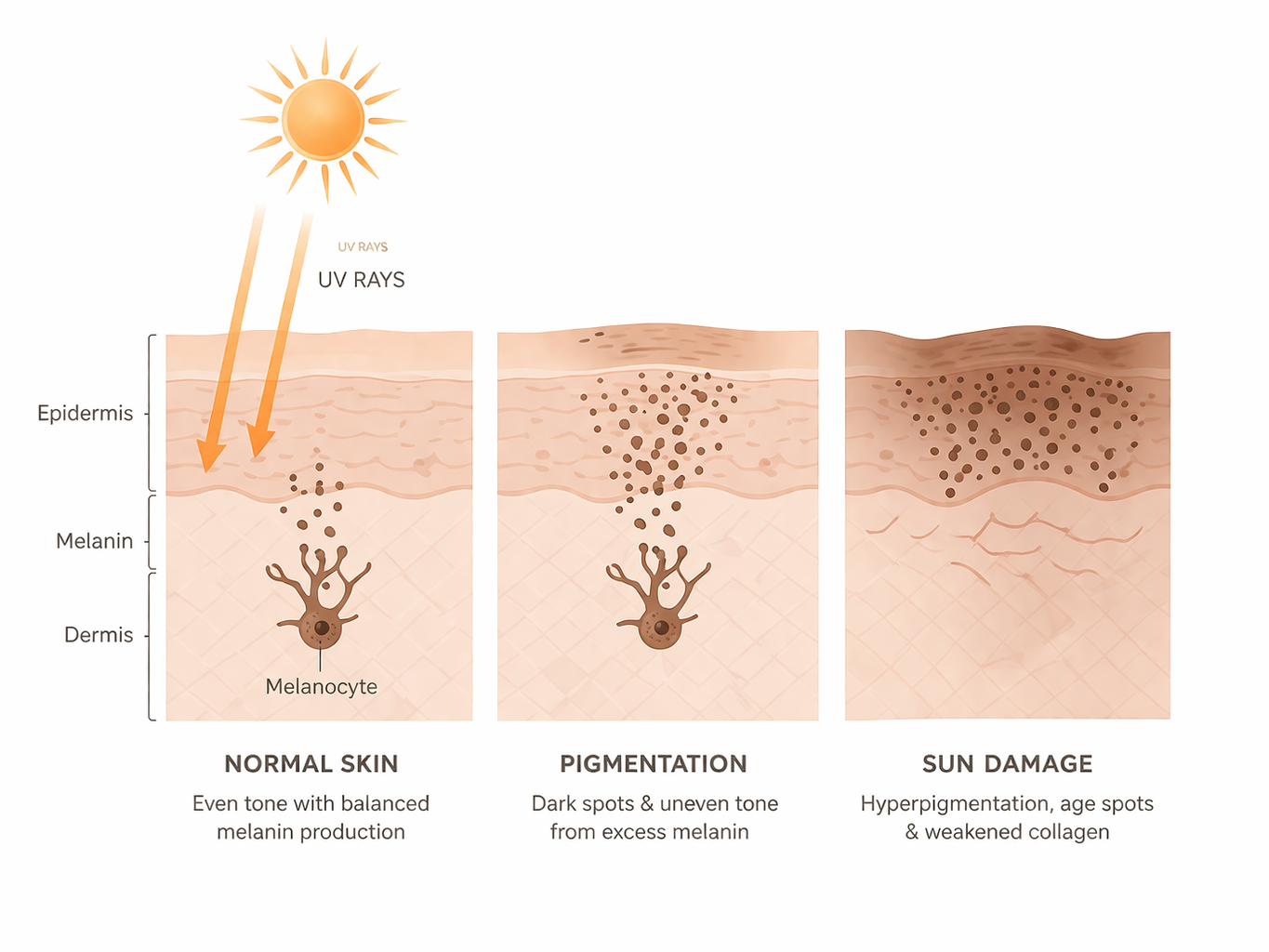
Pigmentation & sun damage

Pigmentation is one of the most commonly mistreated concerns in aesthetic medicine. The reason is simple — it looks like one problem, but it’s almost never just one thing.
Sunspots respond differently to melasma. Post-inflammatory pigmentation triggered by acne needs a completely different approach to UV-driven sun damage. And melasma — which is hormonal, chronic, and stubborn — will return after laser treatment if the hormonal driver hasn’t been addressed first. Treating it without that conversation isn’t just ineffective. It’s expensive and demoralising for the patient.
Assessment here looks at pigmentation type and depth, triggers and history, skin type, and UV exposure patterns before any treatment is planned.
Management may include targeted light or laser therapies, combination approaches for mixed pigment and vascular change, strict photoprotection, and medical-grade skincare. For melasma specifically, long-term management and expectation-setting are part of every plan from the beginning.
Recurrence is common. Maintenance is essential. Anyone who tells you otherwise isn’t being straight with you.